

The sting in the tail: part two
How did a Covid-19 case slip through New Zealand’s quarantine and testing system?

The most important tool for Covid-19 management has always been testing. Knowing exactly who is infected is at the centre of any programme to manage a disease. But the question of who is infected, and who isn’t, is not quite as simple as it first appears.
At what point do we say that a person becomes “infected”? It can’t be the point where they come into contact with the virus – after all, not everybody who comes into contact with the virus actually catches it. It’s not the point where someone shows symptoms of the disease, because people are able to pass the virus onto others before they show symptoms. Somewhere in between those two moments, is there a precise point when we know that someone is infected with the virus?
To know when that precise point of infection occurs, we need to understand the life cycle of viruses – if viruses can be said to have a life cycle, since they aren’t, strictly speaking, alive at all. A virus consists of nothing more than its genetic material – DNA or the similar molecule RNA – and a coating around that genetic material. Viruses have no cells, and they are unable to do anything that a cell, or an organism made up of cells, is able to do. They don’t move, don’t breathe, don’t consume food to give themselves energy, and they don’t excrete any waste products.
What, then, do viruses actually do? If the virus which causes Covid-19 – SARS-CoV-2 – can’t really do anything, how has it infected more than 45 million people, killed around 1.2 million and brought the global economy to a crashing halt.
Although there are many things that a virus can’t do, they have one very specific ability, which is to take over the cells of a living thing – human, bat, plant or even bacteria. Viruses are cellular hijackers. A hijacked cell continues to do all the things a cell normally does, but instead of reproducing itself, it makes copies of the virus.
However, in order to hijack a cell, the virus has to get inside that cell, and in order to do that, the first thing that the virus has to do is find a cell to infect. Since viruses can’t move, they don’t actually do anything to find that cell. Instead, they are carried by something. In the case of Covid-19, the virus is carried in droplets which are sneezed or coughed out of the lungs. Other viruses are carried in different ways – the virus which causes dengue fever is carried by mosquitoes, the polio virus is carried in faecal matter (that is, poo) which gets into water and the Ebola virus is carried in bodily fluids such as blood.
But understanding how a virus is spread only tells half the story. Once a virus carried on a droplet is breathed into a human nose, or a virus carried in blood enters an open wound, it needs to get inside a cell. Again, the virus doesn’t do anything itself. Instead, the coating on the outside of the virus has specific proteins which attach to the surface of the cell. Once attached, the cell sucks the virus inside. To continue with the hijacker analogy, it’s as if the virus has a key, and if it comes across a cell which has the right lock for that key, then the virus simply opens the door, waltzes in and takes over.
The cell, of course, doesn’t have this lock just so that it can get invaded by viruses. The locks have important functions for whatever it is that the cell does. In the case of Covid-19, the virus attaches to cells which have a particular lock (known as a receptor) called ACE2. ACE2 controls one of the body’s hormones, ANG II, which is part of the system which controls blood pressure and fluid balance in the body. Among other things, ANG II tells the brain that we need to drink – it controls the sensation of thirst. ACE2 is embedded in the surface of cells all around the body, including the airways and lungs. When the Covid-19 virus is breathed in, and it lands on cells which have the ACE2 lock, the virus’s “key” means that it gets taken into these cells. Many cells in the gut also have ACE2 locks, and there is increasing evidence that the virus can infect the body this way as well.
Once the virus is inside human cells, the cell treats the virus’s genetic material as if it is the cell’s own. The virus’s genetic material tells the cell to stop doing what it normally does and start making more copies of the virus, which are then released into the body. Once this process is happening, we can definitely say that a person has become infected with that virus.
But what does this mean for Covid-19 testing? We have defined the point where someone becomes infected, but does this mean that a test will tell us that they are infected?
The answer, unfortunately, is “not yet”.
There are two main types of diagnostic test for Covid-19. The first type is a direct test, usually known by the acronym PCR, which stands for polymerase chain reaction. This type of test targets the genetic material of the virus. PCR tests can be incredibly sensitive, because the enzyme polymerase, for which the test is named, multiplies the genetic material which it targets, until there is enough to detect it easily. Back when I was working on viruses, more than 25 years ago now, this type of test was new, exciting, and rather slow and tricky to do. Today, it’s fast, cheap and routine.
The second type of test is an antibody test. This type of test looks for the body’s immune response rather than the virus itself, that is, it looks for the antibodies that we have made to fight the virus. Immediately, there’s an obvious difference with the PCR tests. A PCR test will be effective as soon as there is enough virus in your body for it to be present in the sample taken. But an antibody test will only work once your body has made enough antibodies to fight the virus. It also continues to give a positive result long after the virus is gone from your body. This is a good thing if you want to know who has had the virus in the past, but it’s not a good test to use when making decisions about who needs to be in quarantine.
There’s a good explanation of the the two types of test on our Ministry of Health website. There’s also a graph, which I’ve copied here, because it explains the main issue with both types of test more clearly than any words. What the graph shows is that it takes time for both the PCR test and the antibody test to return a positive result in someone infected with Covid-19.
Levels of virus and antibodies after catching COVID-19 and the likelihood they will be detected during testing. (from New Zealand Ministry of Health)
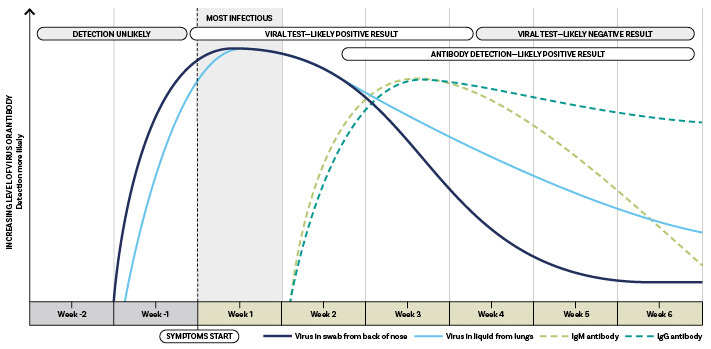
It’s immediately clear, both from the graph, and from how the test works, that an antibody test is almost useless as a part of our border testing regime. Firstly, it takes some time after infection before it indicates someone has the virus – 1-3 weeks according to the US Centres for Disease Control and 2-3 weeks according the New Zealand Ministry of Health. But, most importantly, antibodies stay in your body for some time after you have had an infection, when there’s no chance of you passing on the virus. Since we have known about Covid-19 for less than a year, we don’t know how long that is, but recent evidence suggests that antibodies last months, not years. Still, we clearly wouldn’t want to keep people in quarantine on the basis of an antibody test.
Because the levels of virus in the body increase before the levels of antibodies do, testing directly for the virus, with a PCR test, is far more useful from a quarantine perspective. The PCR test is also much more sensitive, because of the step in the process where the enzyme polymerase multiples the amount of target RNA. But, even then, it’s possible to get a negative test result from someone who is infected with the virus.
Even though PCR tests are extremely sensitive to low levels of virus, there’s still a level which is too low to detect. If someone is showing Covid-19 symptoms, the chances are that there will be enough of the virus present to give a positive result. So, if we test someone who has had a fever and a cough for a couple of days, we can be very confident in the result of the test – if it says they don’t have Covid-19, then they almost certainly don’t. However, if someone had a fever and cough last week, but they are mostly feeling better at the time of testing, a negative result tells us very little. Perhaps they didn’t have Covid-19. Or perhaps they did, but they have fought off the virus and there’s no longer enough left in their body to show up.
Of course, that scenario – figuring out whether someone has had Covid-19 in the past – is exactly what the antibody test does well. So it’s no problem that the PCR test won’t necessarily detect past infections. (Evidence suggests that the PCR test does detect past infection sometimes, just not often enough for it to be used for that purpose.)
The problem, of course, is that none of the Covid-19 tests available are good at detecting the virus early in the infection process. PCR tests can detect Covid-19 before symptoms develop, that is, during the incubation period, but we can’t be confident that they will. We saw a clear example of this in New Zealand’s most recent community case of Covid-19. A worker at an Auckland quarantine hotel underwent a routine test on the 3rd of November, which returned a negative result. On the 5th of November, they developed symptoms and took another test, which was positive. Since the incubation period is usually longer than 2 days, it’s very likely that they were infected when they returned that initial negative test.
It’s not clear exactly when in the infection cycle we can be confident in a negative Covid-19 test. As I mentioned earlier, we know that if someone is tested 2-4 days after they first show symptoms of Covid-19, and the test returns a negative result, we can be very confident that the symptoms are not actually Covid-19. We know this because the tests have been evaluated using known positive samples, and in those cases, it’s rare that tests return a negative result. However, it’s still not impossible. The studies that I have linked to used only 50 positive samples for each test evaluation. If the evaluation has a sensitivity value of 100%, which many do, that simply means that there were no negative results out of 50 positive samples. We don’t know what would happen if a larger number of samples was tested.
Of course, those results assume that the tests are always done correctly. It is possible, and in fact likely, that the people collecting the samples, transporting the samples and testing the samples will occasionally make mistakes. It probably doesn’t happen often, but it’s optimistic, and dangerous, to think that it never happens at all.
But the real problem for our quarantine system is that we don’t know what a negative test means when we test someone who hasn’t had any Covid-19 symptoms. Sometimes it will mean that the person is not infected. And sometimes it will mean that the person is infected, but there isn’t yet enough virus in them to show up in the test. This is why we can’t simply test people as they arrive in New Zealand and then let them go if their test comes back negative. The only thing we can do is wait.
This brings us back to the question of how a Covid-19 case could have slipped through our quarantine system, setting off the cluster which closed down Auckland in August, and infecting 179 people. It’s possible that it slipped through because of mistakes – people who should have been tested but weren’t, or tests which weren’t done properly. But is it also possible that we will still have the occasional case which gets through, even if we do everything right?
We know from the work in Belgium that if we put people in quarantine for 7 days, and then give them a Covid-19 test, we will pick up people who are infected 88% of the time. That’s not good enough for New Zealand to rely on – not if we want to continue enjoying our concerts, sports games and family celebrations without killing a lot of people. It doesn’t even seem that the strategy was good enough for Belgium, a country whose goal with Covid-19 is simply to avoid collapsing the health system. After adopting that strategy for self-isolating contacts in early October, they’ve just gone into another nationwide lockdown.
We know that a small proportion of people who show no symptoms of Covid-19 after 14 days in quarantine will actually be infected, as I discussed in my previous article. Some of these will go on to become sick, perhaps as much as 10 days after they leave quarantine. Some will remain asymptomatic, or have symptoms so mild that they never realised that they have Covid-19. We don’t know exactly what proportion of Covid-19 cases are asymptomatic – wildly varying figures are quoted in the media, but reliable, published studies estimate that the figure in is the range of 10-23%.
We know that we can detect Covid-19 in people who are infected but show no symptoms. After all, we wouldn’t know about asymptomatic infection at all if we hadn’t tested people with no symptoms and got a positive result.
But the hole in our quarantine system remains with one very important point that we simply don’t know. As I stated above, we simply don’t know how often we will miss detecting Covid-19 infection if people are asymptomatic at the time of testing. And there’s no obvious way around this problem. We need to find a number of infected but asymptomatic (or pre-symptomatic) people to test, in order to work out how effective the test is, and whether there is an ideal time to detect asymptomatic infection. And how do we find these infected but asymptomatic people? That’s the point where we find ourselves chasing our tails. Because we need to test them.
This circular point takes us back to whether or not a 14 day quarantine, with testing at days 3 and 12, is good enough. That’s something that science can’t tell us. No matter how precisely we know the effectiveness of the system, someone will always think it should be more stringent, and someone else will think it should be less. What the science does tell us is that, while we are able to enjoy freedoms which are the envy of most of the world, we cannot afford to forget the pandemic.
Do you know someone who might enjoy The Turnstone? Please forward it to them.
Did you receive The Turnstone from a friend? You can subscribe and receive it directly every week.
Do you want to see more of The Turnstone? All of the stories can be found in the archive, here.
Have you found a factual error or typo? Let me know and I’ll correct it in the archive version.